Consensus Clinical Practice Guidelines for Inpatient or Urgent Care Management of Acute New Onset Hypoglycemia in Children
Print | Back to Main Guidelines Listing
Northern California Pediatric Hospital Medicine Consortium
This work is licensed under a Creative Commons Attribution-Noncommercial 4.0 International License
Table of Contents
- Executive Summary
- Inclusion & Exclusion Criteria
- Background
- Diagnosis
- Management
- References
- Appendix I – Initial Evaluation of Hypoglycemia
- Appendix II – Initial Treatment for Hypoglycemia
- Appendix III – Management of Hypoglycemia
Executive Summary
Objectives
- Standardize care of pediatric patients with hypoglycemia in the inpatient or urgent care settings
- Uniform diagnostic approach to critical labs
- Uniform treatment protocol
Recommendations
- Diagnosis (see Appendix 1)
- Any patient with symptoms of hypoglycemia should be screened with a point of care glucose
- Symptoms of hypoglycemia may differ by age group
- Hypoglycemia = serum glucose < 70 (unless < 48 hours old)
- Critical labs should be sent for any patient with serum glucose < 50 (see table)
- Initial Treatment (see Appendix 2)
- Oral therapy: Conscious patients/able to tolerate PO fluids safely
- For infants < 1 year, 10 ml/kg of formula or expressed breast milk (may breastfeed while obtaining glucose-containing fluids)
- For patients > 1 year, 0.3 g/kg (10-20g) of rapidly absorbed carbohydrate
- 4 ounces of juice = approximately 15 g
- IV Treatment: Altered mental status or unable to swallow, or not responding to oral glucose within 15 minutes
- Bolus < 1 month: D10W 3mL/kg
- Bolus > 1 month: D10W 5mL/kg (max 250 mL)
- Measure glucose in 15 mins
- Continuous IV glucose infusion for any patient requiring 2nd IV bolus or after the first IV bolus for patients who presented with AMS, seizure or for patients in whom there is a suspicion for underlying pathology requiring continuous infusion (e.g. refractory vomiting, insulinoma)
- Start at GIR 5, increase as needed (see Appendix 3)
- Hospital Admission: Reasons include inability to maintain normoglycemia orally, unknown cause of hypoglycemia, ingestion of long-acting hypoglycemic agent, inability to maintain glucose >70, need for continuous infusion
- Consultations
- Endocrine: Unknown etiology of hypoglycemia, hypoglycemia unresponsive to glucose administration, or GIR>15
- Toxicology: ingestion of known hypoglycemic agent
Methods
This guideline was developed through local consensus based on published evidence and expert opinion as part of the UCSF Northern California Pediatric Hospital Medicine Consortium
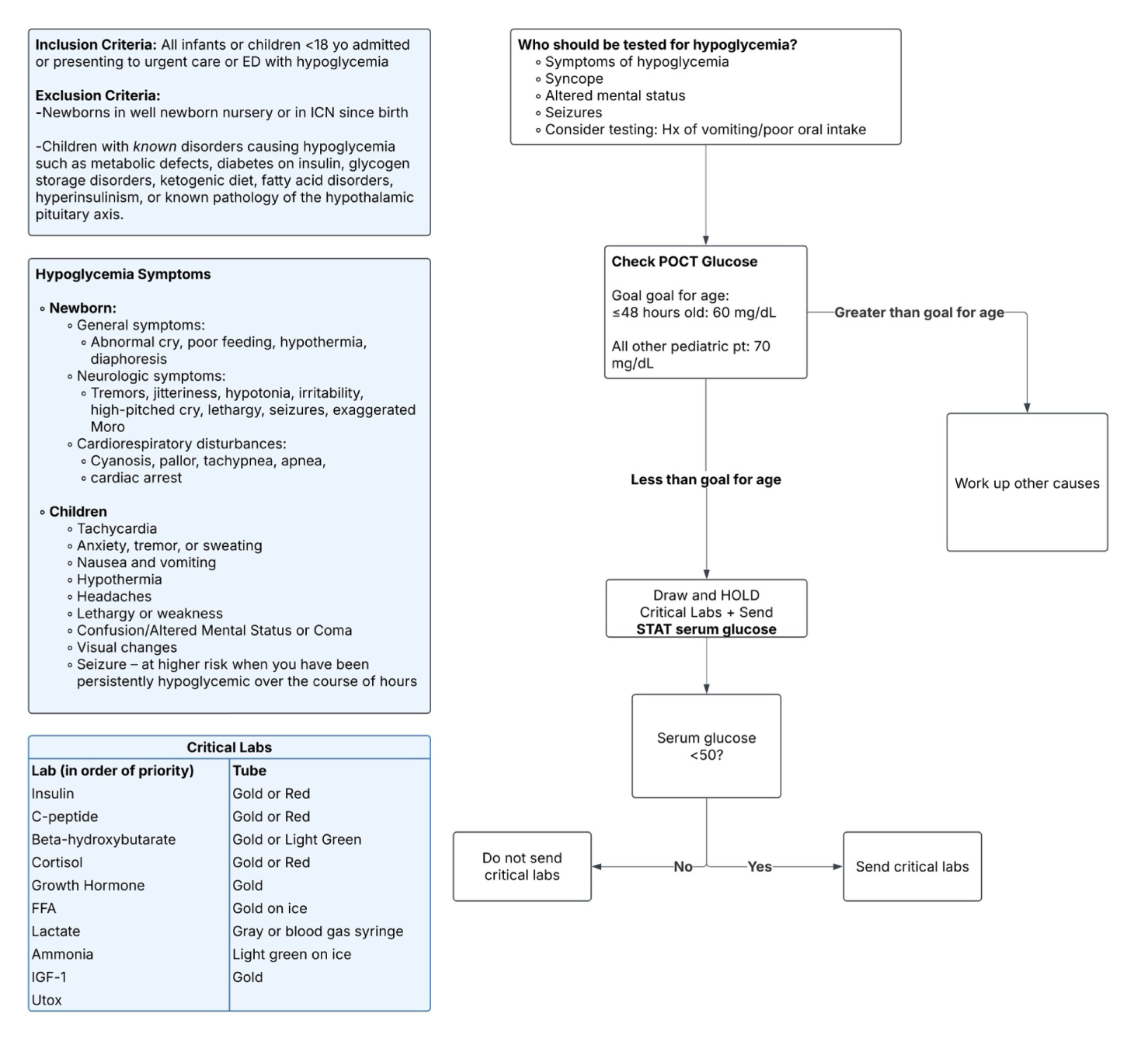
Inclusion Criteria:
All infants or children up to age 18 years admitted or presenting to urgent care or ED with hypoglycemia.
Exclusion Criteria:
- Newborns in well newborn nursery or in ICN since birth
- Children with known disorders causing hypoglycemia such as metabolic defects, diabetes on insulin, glycogen storage disorders, ketogenic diet, fatty acid disorders, hyperinsulinism, or known pathology of the hypothalamic pituitary axis.
Background
- Definition of Hypoglycemia
- Multiple definitions, normative values are different depending on source
- Hypoglycemia with clinical manifestations
- Population data based on standard deviation
- Level at which neurological function is impaired
- Level at which physiologic, metabolic and hormonal shifts occur
- Less than or equal to < 48 hours old: 60 mg/dL
- All other pediatric patients: Less than 70 mg/dL
- Serum blood glucose should be obtained to confirm hypoglycemia since whole blood glucose may be lower than serum glucose.
- Symptoms consistent with hypoglycemia may or may not be present, especially in the newborn period or in chronic hypoglycemia. Symptoms may vary by age.
- Newborn period:
- General symptoms:
- Abnormal cry, poor feeding, hypothermia, diaphoresis
- Neurologic symptoms:
- Tremors, jitteriness, hypotonia, irritability, high-pitched cry, lethargy, seizures, exaggerated Moro
- Cardiorespiratory disturbances:
- Cyanosis, pallor, tachypnea, apnea, cardiac arrest
- Children
- Tachycardia
- Anxiety, tremor, or sweating
- Nausea and vomiting
- Hypothermia
- Headaches
- Lethargy or weakness
- Confusion/Altered Mental Status or Coma
- Visual changes
- Seizure – at higher risk when you have been persistently hypoglycemic over the course of hours
- Causes of hypoglycemia include but are not limited to
- Ketotic Hypoglycemia (Fasting/Starvation) – most common cause
- Transient Neonatal Hypoglycemia
- Hyperinsulinism (transient and congenital)
- Hormone deficiencies (Growth Hormone Deficiency, Cortisol Deficiency)
- Metabolic Disorders (Fatty Acid Oxidation Disorders or Glycogen Storage Disease)
- Toxins
- Medications including insulin
- Sepsis
Diagnosis (See Appendix 1: Initial Evaluation of Hypoglycemia)
- Who should be tested for hypoglycemia?
- Symptoms of hypoglycemia (see above)
- Syncope
- Altered mental status
- Seizures
- Consider testing: Hx of vomiting/poor oral intake
- How to test?
- Point of care glucose
- Any glucose less than goal for age should be confirmed with serum glucose or iSTAT glucose
- Critical Labs: Obtain if glucose is < 50 mg/dL:
- Serum glucose (BMP) STAT
- Draw and HOLD (awaiting confirmation on BMP that serum glucose reflects true hypoglycemia – send if YES)
- In order of priority
*Amount to collect is site specific; please check with local laboratory.
- Other Recommended Lab work (do NOT have to be sent with critical labs during hypoglycemia, can be sent at any time)
- Acyl-carnitine profile
- Free and total carnitine
- Urine Organic Acids
- General Interpretation of Critical Labs

- Glucagon stimulation test (obtain in consultation with Endocrinology – not for initial evaluation of hypoglycemia)
-
- Timing
- After critical sample obtained, reconfirm with POC bedside glucometer that BG < 50 mg/dL. If so, then proceed with glucagon stim testing.
- At time zero, give glucagon 1 mg IV or IM.
- Check POC BG every 10 minutes for 40 minutes
- If at the 20 minute mark, the BG has not risen by at least 20 mg/dL, then stop the test and treat hypoglycemia.
- Interpretation:
- Glucagon stim testing is a sensitive test for detecting hyperinsulinism
- If blood glucose has risen by > 30 mg/dL within 40 minutes in response to glucagon administration, then this is an inappropriate response in the setting of hypoglycemia. This indicates that there is inappropriately stored glycogen.

Management (See Appendix 2: Initial Treatment for Hypoglycemia)
- Treatment: Initial administration of glucose
- PO: Conscious patients/able to tolerate PO fluids safely
- For infants < 1 year, 10 ml/kg of formula or expressed breast milk (may breastfeed while obtaining glucose-containing fluids)
- For patients > 1 year, 0.3 g/kg (10-20g) of rapidly absorbed carbohydrate
- 4 ounces of juice = approximately 15 g
- If unable to take at least 75% of recommended quantity of carbohydrate-containing fluids in 15 mins, proceed to IV
- Recheck in 15 mins
- If glucose < 50 consider placing IV while offering PO treatment; if <30, place IV regardless of ability to tolerate PO and offer PO treatment while obtaining IV
- IV Treatment: Altered mental status or unable to swallow, or not responding to oral glucose within 15 minutes
- Bolus < 1 month: D10W 3mL/kg
- Bolus > 1 month: D10W 5mL/kg (max 250 mL)
- Measure glucose in 15 mins
- Max bolus: 250 mL
- Options if difficulty obtaining IV
- NG tube (particularly in young infant, consider prior to IV)
- Glucagon
- < 5 yo: 0.5 mg IM
- > 5yo: 1 mg IM
- Measure glucose in 15 mins as effects can be transient
- If first dose ineffective, likely child has too few glycogen stores for glucagon to be effective; do NOT give second dose in this situation
- Otherwise, if first dose is effective, can give up to 2 doses
- Intraosseous
- Monitoring
- If repeat glucose still < 70 (or < 60 in first 48 hours of life), give an IV glucose bolus and recheck in 15 mins.
- Otherwise, if glucose is greater than or equal to 70 (or >=60 in first 48 hours of life), check in 1 hour.
- After one hour repeat check, once is > 70, space glucose checks to q3 hours for minimum of 4 hours (goal glucose >70 mg/dL).
- When and How to start a continuous IV infusion (See Appendix 3: Management of Hypoglycemia)
- Start an infusion for any patient requiring 2nd IV bolus
- Start an infusion after the first IV bolus in the following clinical situations:
- Initial presentation with AMS or seizure
- Suspicion for underlying pathology that would lead to inability to maintain blood glucose above goal (refractory vomiting, insulinoma, etc)
- Use dextrose-containing fluids at GIR to maintain BG>70 mg/dL
- Choice of fluids:
- Usually D5 with appropriate sodium content for age
- GIR calculator: https://phillypeds.org/endo/gir
- [% Dextrose x Rate (cc/hr) ]/ (Weight kg x 6 )
- Starting point: GIR of 5
- Note: For older patients >30kg, may need to run a rate higher than maintenance
- Consider using more concentrated dextrose fluids in any patient with fluid sensitivity, e.g. renal or cardiac patients
Initial Fluid Management
*D12.5 is the maximum concentration allowed for peripheral IV administration.
- Increase GIR by 1-2 points at a time if unable to maintain BG above goal and recheck glucose within 30 mins after increasing GIR until stable above goal x2
- Consider additional bolus if glucose remains under 40 while on continuous infusion in addition to increasing GIR as above
- Hospital Admission
- Cannot maintain normoglycemia with oral intake
- Hypoglycemia of unknown cause
- Ingestion of certain long-acting hypoglycemic agents
- During observation, patient cannot maintain glucose >70
- Requiring continuous glucose infusion
- Monitoring for patients on continuous infusion who have achieved normoglycemia
- Check q3 hours while on continuous infusion
- Weaning
- Ability to wean will depend on clinical scenario; for rare pathologies, consult Endocrinology
- Wean 1-2 GIR points every 3 hours as clinically tolerated
- Hospital Discharge Criteria
- Reasonable explanation for initial hypoglycemia
- Able to maintain normoglycemia (glucose >70) on PO fluids for clinically appropriate amount of time
- Consultations
- Endocrinology consultation
- Unknown etiology of hypoglycemia
- Hypoglycemia not responsive to glucose administration
- Requiring GIR >15 to maintain glucose above goal
- Toxicology consultation
- For patients who ingested known hypoglycemia causing agent
References
Ghandi, K. (2017). “Approach to Hypoglycemia in infants and children.” Transl Pediatr 17;6(4):408-420
Institutional Pathways/Guidelines:
- Children’s Hospital of Philadelphia
- MGH
- Ohio State University
Appendix I – Initial Evaluation of Hypoglycemia
Appendix II – Initial Treatment for Hypoglycemia

Appendix III – Management of Hypoglycemia

Disclaimer
These clinical practice guidelines are based upon the evidence-based consensus opinions of consortium members affiliated with UCSF Benioff Children's Hospitals. They are intended to guide pediatric/neonatal providers, but do not substitute for individual clinical judgment. Evaluation and treatment of specific patients should be adapted based upon the unique conditions of each patient, family and clinical environment.
UCSF Northern California Pediatric Hospital Medicine Consortium. Initiated 3/2018. Last updated 6/2025.
Approved by UCSF P&T Medication Subcommittee: 8/13/19
Approved by UCSF Pharmacy and Therapeutics Committee 6/202

